

The 9/29 issue of the ISMP Medication safety Alert! included an URGENT REQUEST for action regarding confirmed mix-ups between Prolia and Udenyca syringes.
************************************
ISMP has learned of two serious medication errors involving the administration of UDENYCA (pegfilgrastim-cbqv; Coherus BioSciences) instead of PROLIA (denosumab; Amgen). Udenyca is a biosimilar leukocyte growth factor associated with the reference pegfilgrastim product, NEULASTA, and Prolia is an osteoporosis drug. Both of these errors were reported to the US Food and Drug Administration (FDA). Prior to these cases, ISMP had received 13 reports of concerns about potential mix-ups or close calls in which the wrong product had been dispensed or retrieved from stock; however, until now, the errors never reached the patient.
In the first case, an 80-year-old male patient with osteoporosis accidently received Udenyca instead of Prolia. Barcode scanning did not occur when retrieving the medication from the refrigerator or before administration. Although the patient appeared to be fine after receiving the wrong drug and was sent home, 1 day after the error, the patient experienced chest pain and presented to the emergency department. The patient’s troponin increased from 0.07 ng/mL to 0.25 ng/mL in 8 hours and his white blood cell count had gone from 4,700/mm3 to 25,800/mm3. The patient was subsequently admitted to the hospital with a diagnosis of non-ST segment elevated myocardial infarction (non-STEMI).
In the second case, a patient at a general infusion center received a single dose of Udenyca instead of the prescribed Prolia. The error was identified when a different patient in the infusion center was to receive Udenyca, and the nurse realized that she still had a carton of Prolia in stock, but not the needed Udenyca. The patient was subsequently contacted and made aware of the error. The patient reported experiencing bone pain following the Udenyca injection but had no other complaints. During Udenyca clinical trials, the most common adverse reactions were bone pain and pain in the extremities.
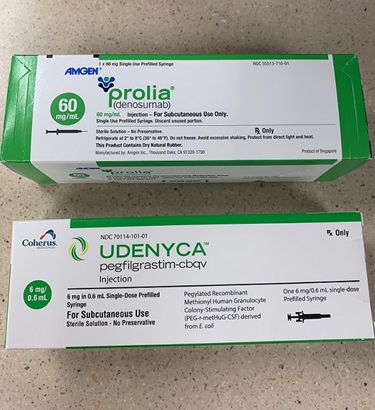
ISMP previously alerted readers to the potential for mix-ups in the May 23 and July 18, 2019, issues of the ISMP Medication Safety Alert! Both medications look similar with green and white packaging, and the concentration is listed in a green circle in the same location (see attached photo). Each carton holds one single-dose, prefilled syringe, and both medications are intended for subcutaneous administration. The Prolia 1 mL syringe contains 60 mg, and the Udenyca 0.6 mL syringe contains 6 mg. Once the carton is opened, the syringes look different. Prolia and Udenyca are likely to be dispensed to the same outpatient oncology centers and infusion centers. Both are refrigerated items and may be near one another, especially if stored alphabetically by brand name.
Earlier, ISMP discussed the risk of mix-ups with Coherus BioSciences and FDA, and we understand that packaging changes are actively being pursued. ISMP urges pharmacists and other healthcare practitioners to ensure that inventories of these products are stored away from one another and that barcode verification occurs whenever possible before dispensing and administering the drugs. Pharmacy staff are also urged to apply a prominent auxiliary label to the outer carton that warns against confusion. Pharmacists should also consider circling (with a permanent marker) the drug name on the carton to draw attention to it.
{kind=link}